Tireoidectomia Total Sem Esternotomia para um Gigante Bócio Retrosternal com Ocorrência Simultânea de Dois Carcinomas de Tireoide: Resultados e Abordagem Cirúrgica
Barra lateral de artigos
Conteúdo do artigo principal
Resumo
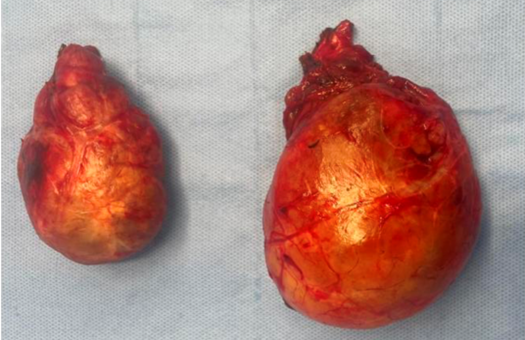
Os bócios retroesternais frequentemente provocam sintomas compressivos, como dispneia, disfagia e sensação de plenitude cervical, além de apresentarem desafios cirúrgicos significativos. O tratamento padrão é a tireoidectomia total, embora a necessidade de esternotomia dependa do tamanho e da extensão do bócio. Apresentamos o caso de uma mulher de 51 anos com massa cervical anterior progressivamente crescente. A imagem revelou lobos tireoidianos significativamente aumentados com extensão retroesternal, causando desvio e estreitamento traqueal. A tomografia computadorizada (TC) mostrou nódulos heterogêneos com componentes císticos, necróticos e calcificados; os lobos mediam 13×7×8,2 cm e 8,3×4,6×5,1 cm. Não foi observada linfadenopatia. A paciente foi submetida à tireoidectomia total por meio de incisão cervical de 6 cm, utilizando dissecção e manipulação cuidadosas, apesar da profunda extensão intratorácica. A patologia macroscópica revelou cápsulas intactas, e a histopatologia mostrou um carcinoma colisionante da tireoide: carcinoma folicular minimamente invasivo (pT3a, pN0a) no lobo esquerdo e carcinoma oncocítico encapsulado e angioinvasivo (pT1b, pN0a) no lobo direito. No pós-operatório, a paciente apresentou hipoparatireoidismo transitório, resolvido com suplementação de cálcio. Este caso destaca a viabilidade de realizar tireoidectomia total em bócios retroesternais gigantes sem esternotomia, mesmo quando o bócio se estende até o hilo pulmonar. Evitar a esternotomia minimiza riscos perioperatórios e o tempo de recuperação. A histopatologia revelou carcinomas diferenciados sincrônicos de origem folicular, ressaltando a importância da ressecção completa em bócios retroesternais.
Detalhes do artigo

Este trabalho está licenciado sob uma licença Creative Commons Attribution 4.0 International License.
Authors retain the copyright of their articles and grant the journal the right of first publication under the Creative Commons Attribution (CC BY) license, which allows others to share and adapt the work with proper attribution.
Referências
Rui Sheng Y, Chong Xi R. Surgical approach and technique in retrosternal goiter: Case report and review of the literature. Annals of Medicine and Surgery. 2015;5:90.
Coskun A, Yildirim M, Erkan N. Substernal Goiter: When is a Sternotomy Required? Int Surg. 2014;99:419.
Rugiu MG, Piemonte M. Surgical approach to retrosternal goitre: do we still need sternotomy? Acta Otorhinolaryngologica Italica. 2009;29:331.
Wang X, Zhou Y, Li C, Cai Y, He T, Sun R, et al. Surgery for retrosternal goiter: cervical approach. Gland Surg. 2020;9:392–400.
Polat ŞB, Arpacı D, Yazgan A, Başer H, Kılıç M, Ersoy R, et al. Simultaneous occurrence of different follicular neoplasms within the same thyroid gland. Turkish Journal of Endocrinology and Metabolism. 2016;20:31–5.
Hao Z, Cui H, Li Y, Wu W, Wang Y, Dan H, et al. Simultaneous occurrence of papillary thyroid carcinoma, medullary thyroid carcinoma, and lymphoma: A case report. Medicine (United States). 2024;103:e39363.
Cichoń S, Anielski R, Konturek A, Baczyński M, Cichoń W, Orlicki P. Surgical management of mediastinal goiter: Risk factors for sternotomy. Langenbecks Arch Surg. 2008;393:751–7.
Huins CT, Georgalas C, Mehrzad H, Tolley NS. A new classification system for retrosternal goitre based on a systematic review of its complications and management. International Journal of Surgery. 2008;6:71–6.
De Perrot M, Fadel E, Mercier O, Farhamand P, Fabre D, Mussot S, et al. Surgical management of mediastinal goiters: when is a sternotomy required? Thorac Cardiovasc Surg. 2007;55:39–43.
Torre A, Varanda J, Castro B, Graça S, Póvoa A, Soares C, et al. Diagnostic Accuracy Study of CT Scan in Predicting the Need for Sternotomy in Management of Substernal Goiters. World Journal of Endocrine Surgery. 2021;13:37–41.
Nankee L, Chen H, Schneider DF, Sippel RS, Elfenbein DM. Substernal goiter: when is a sternotomy required? J Surg Res. 2015;199:121.
Cohen JP. Substernal goiters and sternotomy. Laryngoscope. 2009;119:683–8.
Linhares SM, Scola WH, Remer LF, Khan ZF, Nguyen DM, Lew JI. Depth of mediastinal extension can predict sternotomy need for substernal thyroid goiters. Surgery (United States). 2022;172:1373–8.
White ML, Doherty GM, Gauger PG. Evidence-based surgical management of substernal goiter. World J Surg. 2008;32:1285–300.
Testini M, Gurrado A, Avenia N, Bellantone R, Biondi A, Brazzarola P, et al. Does mediastinal extension of the goiter increase morbidity of total thyroidectomy? A multicenter study of 19,662 patients. Ann Surg Oncol. 2011;18:2251–9.
Prete FP, De Luca GM, Sgaramella LI, Pasculli A, Di Meo G, Testini C, et al. Prevalence and Clinical Risk Factors of Thyroid Cancer in Retrosternal Goiter: A Retrospective Comparative Study with Cervical Multinodular Goiter. Journal of Clinical Medicine. 2025;14:489.